This is the written document to accompany my YouTube video: https://www.youtube.com/playlist?list=PLr1wI57Ez8GQuRAOyFpYclp1pE0WkJisq
While reading this document, it will be beneficial to download a copy of the current edition of the Official ICD-10-CM Coding Guidelines from www.CMS.gov

Purpose:
The purpose of the ICD-10-CM Coding Guidelines is to provide a standardized set of rules and instructions for assigning medical codes to diagnoses. This ensures consistency and accuracy in medical coding by guiding healthcare providers and coders on how to properly select the most appropriate diagnosis codes based on patient documentation. Ultimately, this facilitates accurate billing, data analysis, and communication across healthcare systems.
These guidelines have been developed to assist the healthcare provider and the coder in identifying the diagnoses to be reported. The importance of consistent, complete documentation in the medical record cannot be overemphasized. Without such documentation, accurate coding cannot be achieved.
Why do we assign codes for diagnoses and procedures? The number one reason is confidentiality! Unless you are a trained medical coder, when you view a patient’s medical record and the diagnosis is identified with a code, you won’t know what that code stands for. However, there are other reasons as well. For example, to identify patterns in disease and treatment, develop new treatments, and improve the quality of healthcare.
If you have not reviewed Part 1, go back and review that first, and then continue your review of the 2025 Official ICD-10-CM Coding Guidelines here.
Let’s continue our review of these ICD-10-CM Official Guidelines for Coding and Reporting.
B. B. General Coding Guidelines
1. Locating a code in the ICD-10-CM
There are 3 steps to coding:
- Locate the main term in the Alphabetic Index
- Verify the code in the Tabular List
- Assign the “verified” code
*So, how do you locate a main term in the Alphabetic Index?
The main term describes the condition of the patient. It is NOT the body part. Ex. Breast Mass
The main term in “Breast Mass” is: ___Mass_____________
The main term is in bold print, starts with a capital letter, and is farthest to the left.
So, based on the condition “Breast Mass”, I would look up “Mass”
Subterms are indented to the right under the main term in regular type and with a lowercase letter.
So, based on the condition “Breast Mass”, I would look for “breast” under the main term “Mass”
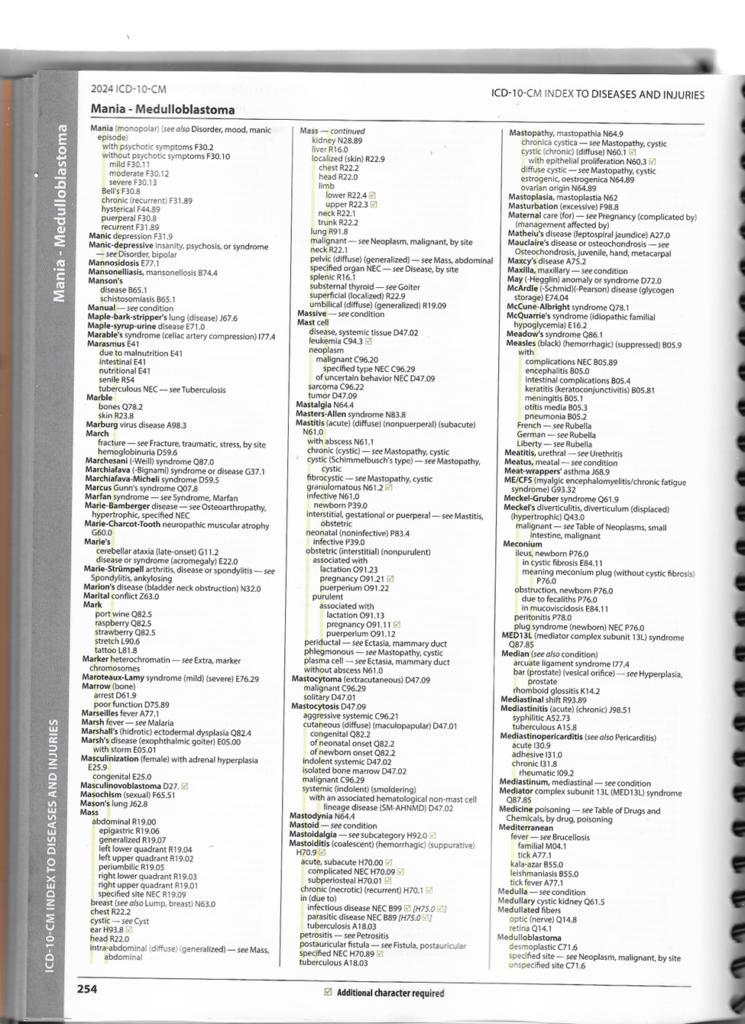
If I needed even more specificity, some subterms have additional subterms indented further to the right under the previous subterm. (I call these sub-subterms)
Example: Main Term: “Mass”, subterm: Abdominal, sub-subterm: epigastric
(refer to previous Alphabetic Index page – “Mass”)
The Alphabetic Index does not always provide the full code. Selection
of the full code, including laterality and any applicable 7th character can only be done in
the Tabular List. A dash (-) at the end of an Alphabetic Index entry indicates that
additional characters are required. Even if a dash is not included in the Alphabetic Index
entry, referring to the Tabular List is necessary to verify that no 7th character is required. (Refer to Main Term: Mass, subterm: ear H93.8(box with a check in it))
View H93.8 Tabular List Below:
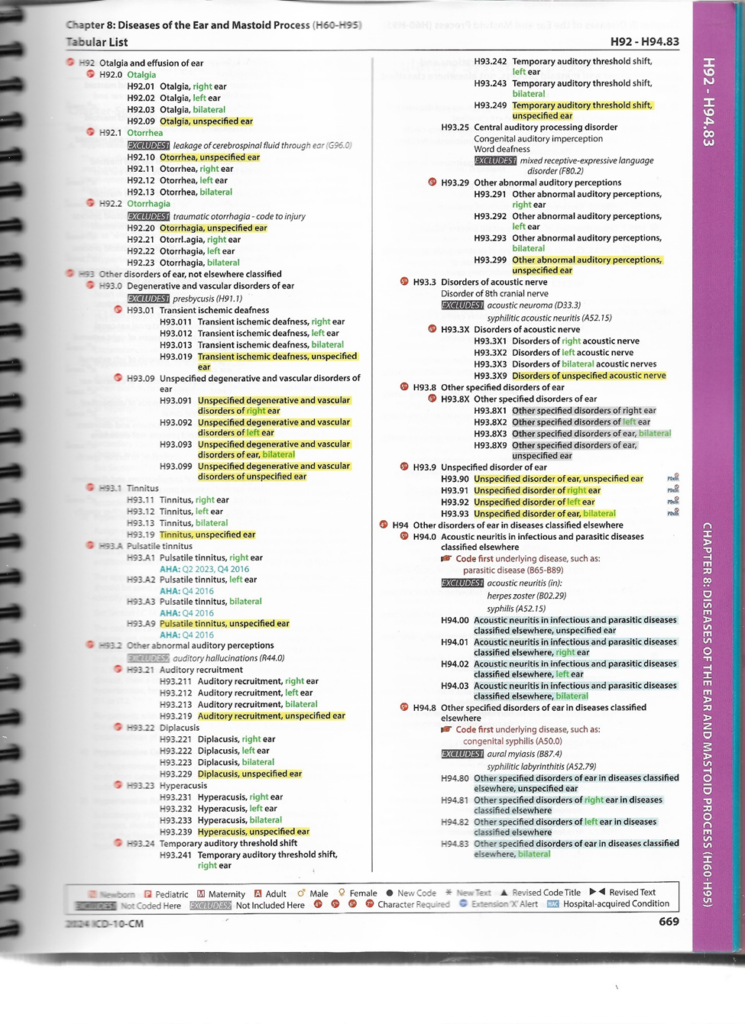
2. Level of Detail in Coding – Refer to Guidelines and then H93.8 above
3.Code or codes from A00.0 through T88.9, Z00-Z99.8, U00-U85 – Straight from Guideline.
4. Signs and symptoms –
Symptom: Observed by “patient”
Sign: Observed by “physician”
5. Conditions that are an integral part of a disease process – Refer to Guideline.
6. Conditions that are not an integral part of a disease process – Refer to Guideline.
7. Multiple coding for a single condition – Refer to Guideline: paragraphs 1 & 2 then N39.0 Below

Code First: “Diabetic Retinopathy”
“Code, if applicable, any causal condition first”: (Ex. Insomnia due to a medical condition)

8. Acute and Chronic Conditions: (Refer to Guidelines)
What is the difference between “acute” and “chronic”?
Acute is: immediate, happening now, urgent
Chronic is: ongoing, not immediate, long-term
9. Combination Code – (Refer to Guidelines)
Example: “Canaliculitis”, acute and chronic



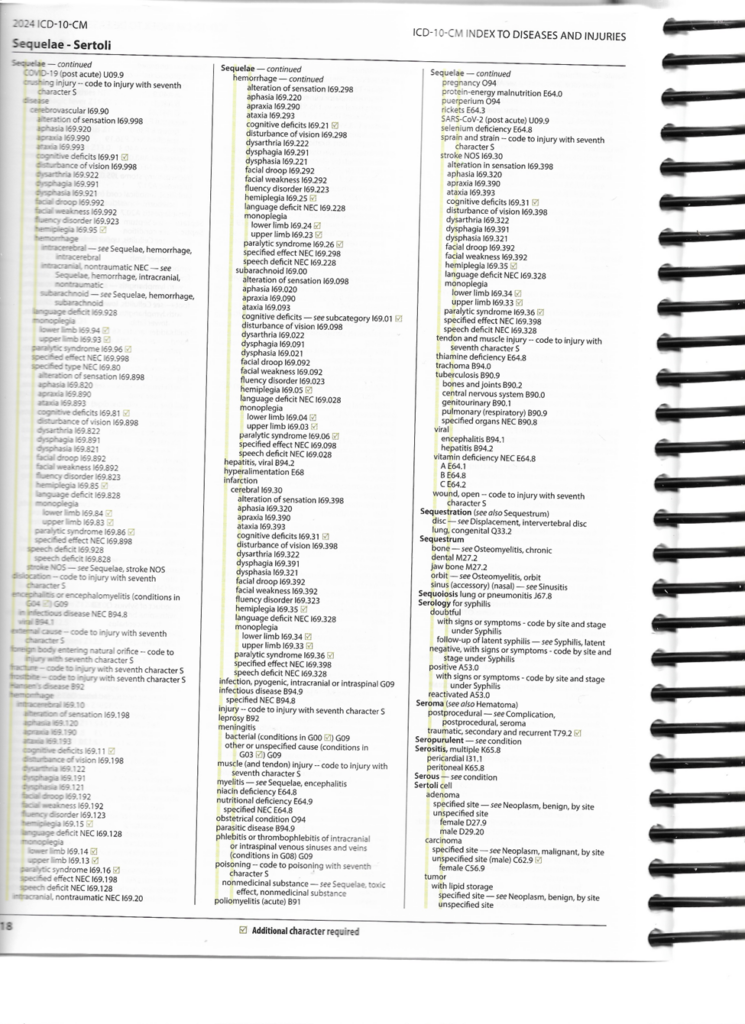
10. Sequela (Late Effects) – Refer to Guideline
A “sequela” is the result of something. For example, a “scar” is a result of a burn.
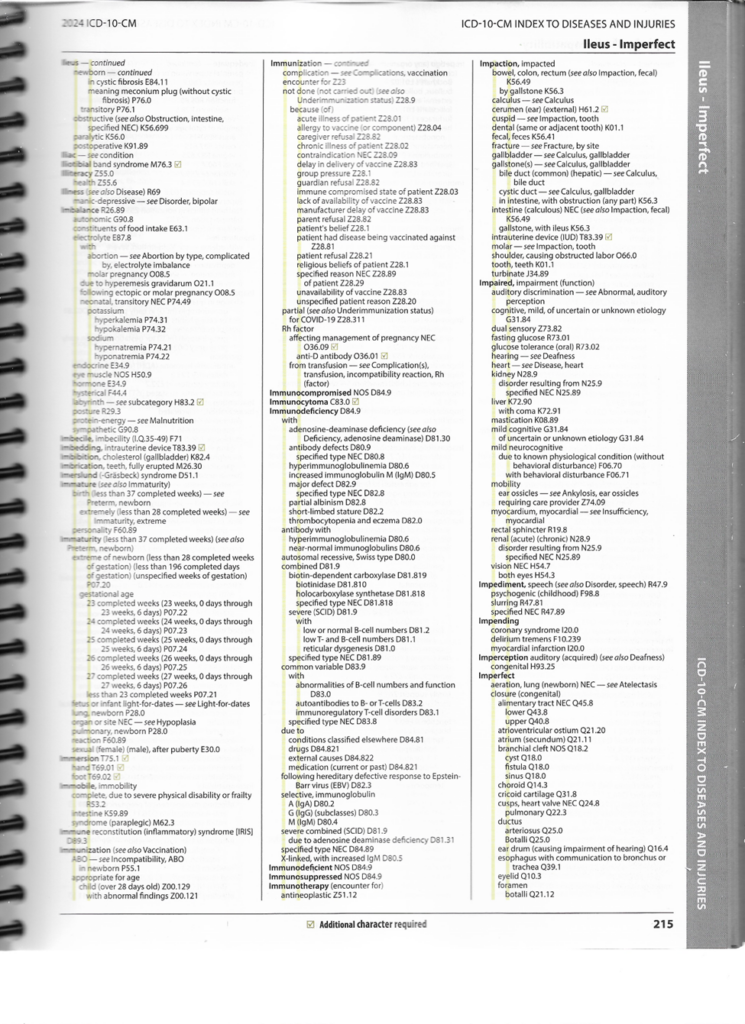
11. Impending or Threatened Condition – Refer to Guideline.
12. Reporting Same Diagnosis Code More than Once – Refer to Guideline. (clear)
13. Laterality – Refer to Guideline.
14. Documentation by Clinicians Other than the Patient’s Provider – Refer to Guideline.
15. Syndromes – Refer to Guideline, then page below.

16. Documentation of Complications of Care – Refer to Guideline.
17. Borderline Diagnosis – Refer to Guideline. Then, main term: “Borderline”

18. Use of Sign/Symptom/Unspecified Codes – Refer to Guideline. (straight to the point)
19. Coding for Healthcare Encounters in Hurricane Aftermath – Refer to Guideline.
- Use of External Cause of Morbidity Codes – (How, Activity, Place & Status)
- Sequencing of External Causes of Morbidity Codes
- Other External Causes of Morbidity Code Issues
- Use of Z-codes
These guidelines are so long that it will take more than one blog post to cover them fully. Please refer to the continuation as I add them.
Don’t forget to download a copy of the Official ICD-10-CM Guidelines here: www.CMS.gov
as well as follow along on my YouTube at: https://www.youtube.com/playlist?list=PLr1wI57Ez8GQuRAOyFpYclp1pE0WkJisq